Life Extension Magazine®

Heart Attack Makes Deadly Comeback
Cardiovascular deaths are rising due to surging rates of obesity and diabetes. Comprehensive blood tests can identify risk factors before the onset of irreversible disease.
Scientifically reviewed by: Dr. Gary Gonzalez, MD, in August 2023. Written by: William Faloon.

Do you remember how prevalent heart attacks and strokes used to be in the 1960s?
Acute cardiovascular death was so common that corporations faced management crises as key executives perished from heart attacks.
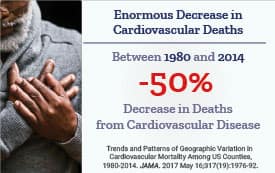
One of medicine’s great achievements has been slashing deaths from heart attack and stroke.
The slides on this page demonstrate remarkable decreases in cardiovascular deaths that have occurred in recent decades.
I use these slides in live presentations to demonstrate how technology is winning the war against degenerative aging.
Sadly, a prediction made by many experts has transformed into tragic reality.
Instead of cardiovascular deaths continuing to plummet as they have over the past 60 years, they are increasing in middle-aged Americans.
In some cases, older parents today are seeing their middle-age children perish from preventable vascular disorders.
The reasons are not surprising.
An underlying cause is an obesity and type II diabetes epidemic that is offsetting robust gains made against cardiovascular diseases in past decades.
The encouraging news is that aging individuals can garner significant protection by following proven cardiovascular risk reduction behaviors.
Those who fail to measure and correct artery-clogging factors are at high risk of heart disease and stroke.
Life Extension® readers have annual blood tests to take corrective actions before chest pain, paralysis, or death b arterial blockage manifests.
This article provides a wealth of published data about how to slash one’s risk of suffering a crippling or lethal cardiovascular event.
America’s heart attack epidemic peaked in 1968 and steadily declined as more people understood the artery-clogging role of poor dietary and lifestyle behaviors.
Cardiovascular risk plummeted in response to:1-7
- Sharp drop in tobacco use,
- Improved emergency responses,
- Near perfection of angioplasty and stenting,
- Huge drop in LDL-related blood lipids resulting from changes in dietary patterns and advancements in pharmacology,
- Use of aspirin for secondary prevention (reduction in heart attack or stroke after having had a prior event), and
- Reduced systolic blood pressure targets.
There has also been a 20-fold increased intake of dietary supplements (like vitamin D and CoQ10).
In a remarkable accomplishment, cardiovascular disease mortality declined by around 70% over the past 60 years.7-10
This trend of reduced cardiovascular mortality has now turned in the wrong direction.
The prime culprit is record numbers of American adults who are overweight or obese. This has translated into…
Age-Adjusted Prevalence of Obesity and Diagnosed Diabetes Among U.S. Adults
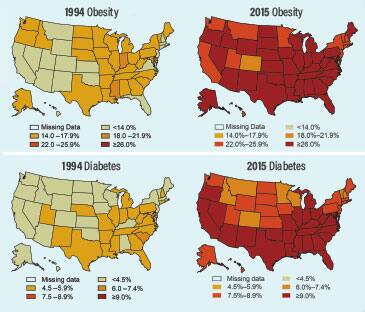
These maps reveal striking increases in obesity (BMI >30 kg/m2) and diabetes that occurred between 1994 and 2015. This is not mere correlation but reflective of the causative impact of excess body weight on one’s ability to maintain optimal (lower reference range) fasting insulin and glucose blood levels.
The material is available on the agency website at no charge.
Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Content source: Centers for Disease Control and Prevention. https://www.cdc.gov/diabetes/statistics/slides/maps_diabetesobesity_trends.pdf
A Resurgence of Cardiovascular Disease
Instead of continuing to decline in prevalence, we are seeing progress grind to a virtual halt.
For people aged 45 to 64, cardiovascular mortality increased during the years 2011 to 2017.11 This death rate increase represents a reversal of what had been sharp declines in heart attacks and ischemic strokes that occurred in previous decades.
These deadly trends correlate with rising levels of obesity, type II diabetes and blood pressure. Here are current statistics in the United States:12-14
- Approximately 40% of adults are clinically obese.
- Over 30% are overweight.
- Approximately 10.5% of adults have diabetes, and
- More than 20% of those with diabetes don’t know they have it.
- Approximately 46% of American adults have hypertension often caused by excess body weight.
The reprint on the left side page shows maps from the Centers for Disease Control and Prevention.
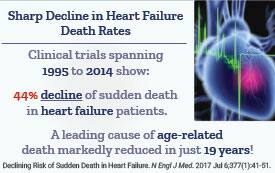
More Heart Failure Deaths
Deaths from heart failure began a steep decline 25 years ago but began surging higher nine years ago as the population ages and the health of younger individuals worsens.
Between 2011 and 2017, the death rate from heart failure increased 20.7% and will likely keep climbing sharply, according to a study published in the JAMA Cardiology.21
The study attributed the resurgence in heart failure deaths to the aging population, along with higher rates of obesity and diabetes, including in people under age 65.
They depict an outbreak of obesity and type II diabetes beginning in 1994 whose impact on cardiovascular disease incidence is now manifesting into deadly reality.
A Ticking Time Bomb
What the maps on the facing page don’t reveal is the number of undiagnosed diabetics, which is astronomical based on today’s surging obesity epidemic.
These maps also don’t consider a position that Life Extension® took in the early 1980s that the concept of "prediabetes" is highly misleading.
That is because damage to eyes (retinopathy), kidneys (nephropathy), and nerves (neuropathy) begins before the onset of full-blown diabetes.
Our position has been validated in dozens of studies showing that damage to blood vessels, nerves, kidneys, and eyes accumulates wit suboptimal glycemic control before full-blown type II diabetes is diagnosed.15-20
To put this into numerical perspective, conventional medicine guidelines in the 1980s diagnosed type II diabetes when fasting glucose reached 140 mg/dL (on two occasions).
Life Extension® vehemently argued that any fasting glucose reading over 100 mg/dL increased one’s risk of developing diabetes, as well as silent damage to blood vessels, nerves, eyes, and kidneys.
For decades, we urged our readers to keep their fasting glucose between 70-85 mg/dL.
Obesity Surges
A startling 72% of Americans are overweight or obese.12
The average person’s glycemic blood markers (hemoglobin A1c, insulin and glucose) today are at frighteningly high levels.
I analogize this ticking diabetic time bomb to how lung cancer deaths did not sharply increase until 30 years after cigarette smoking became prevalent after year 1900.
We are now about 27 years into a spiraling rise of obesity prevalence. The pathologic impact is being demonstrated by increased heart disease deaths in middle-aged Americans.22
You don’t have to be a victim, even if you are in the diabetic or overweight category.
Simple Steps Yield Huge Benefits
In response to the plague of diabetic disorders striking Americans, several studies were initiated to evaluate whether cardiovascular events could be reduced with modest risk-factor changes.
Cigarette Mortality Trends Relate to Today's Obesity Crisis
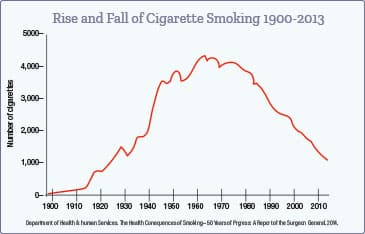
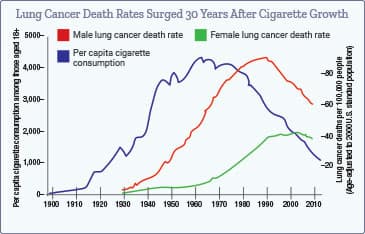
Cigarette smoking was rare before year 1900, but sharply increased thereafter. Lung cancer deaths did not begin to surge until around 1930 and continued increasing up until 1990.
The delay in lung cancer deaths (from 1900 to 1930) occurred while cigarette-smoking rates were surging. The situation reversed when cigarette smoking began declining around 1965, but lung cancer deaths kept rising and did not peak until around 1990. These delays reflect the number of years required for cigarette smoking to cause lung cancer. There are also adverse effects of prior smoking on lung cancer incidence.
A similar situation exists today with overweight and obese individuals who face short- and long-term health issues because of their excess weight.
When only aggressive glycemic control is instituted in type II diabetics, there are usually negligible reductions in heart attack and stroke risk.
This is not surprising when considering that a diagnosis of diabetes often occurs with other co-morbid conditions like hypertension and elevated lipids.
Published data show that when diabetics control other risk factors, like high blood pressure and elevated LDL cholesterol, there are marked reductions in cardiovascular risk.
For example, a group of 2,018 diabetics were treated to achieve safer ranges of blood pressure, hemo-globin A1c (blood marker of long-term glucose control) and LDL cholesterol.23
In those who achieved one or more of the three targeted ranges of:
- Blood pressure
- LDL cholesterol
- Hemoglobin A1c…
…there was an incremental lower adjusted rate of cardiovascular events. In other words, with each additional treatment goal met, cardiovascular risk decreased further.
The chart below shows the percent of risk reduction in response to targeting one risk factor (such as blood pressure),two risk factors, or all three risk factors (blood pressure, LDL, and hemoglobin A1c) vs. none:

This table shows a 60% coronary-event risk reduction when all three risk factors are controlled.
This prompted the study’s authors to note how uncommon it is for diabetics to have all three risk factors in safe ranges.
They concluded that optimization of these risk factors is:
"…associated with substantially lower risk of coronary heart disease and cardiovascular disease."
Cardiovascular disease events include stroke and heart attack.
This study indicates that many lives can be spared if basic, conventional risk factors, especially blood pressure and lipids are better controlled.
Critical Need of Comprehensive Therapy
There is a lack of consistent data on treating diabetics with intensive glycemic control alone.
While aggressive glycemic control by itself lowers risk of kidney failure, neuropathy, and retinopathy, the risk of heart attack and stroke are typically not reduced.
For example, a clinical trial of Danish type II diabetics compared intensive multi-modal therapy to conventional therapy for a mean treatment period of 7.8 years.24

The intensive, omprehensive therapy group had a 57% reduction in cardiovascular disease death and a 59% reduction in cardiovascular disease events.
A much larger, five-year study of 859,617 diabetic adults in the United States showed inadequate risk factor control to be responsible for 11% to 34% of cardiovascular disease events.25
The defined “risk factors” in this five-year study were blood pressure, LDL, hemoglobin A1c, and smoking.
Another study looked at similar risk factors for American type II diabetics and projected that controlling all of them would prevent35% of coronary heart disease events in men and 45% in women.26 The authors concluded:
"…a significant proportion of coronary heart disease events in adults with type II diabetes could be prevented from composite control of risk factors often not at goal."26
The data relating to heart attack and stroke prevention reveal that diabetics need to control more than just glucose and hemoglobin A1c levels.
What About Obese Individuals?
In a 2016 report published in JAMA, Johns Hopkins researchers followed a group of 13,730 people for about 23 years.27
Body Mass Index of this large study group ranged from normal weight (BMI 18.5 to <25 kg/m2) to severely obese (equal to or more than 35 kg/m2).
After controlling for factors like age, smoking status, and physical activity, severely obese subjects had about a two-fold higher risk of coronary heart disease and ischemic stroke.
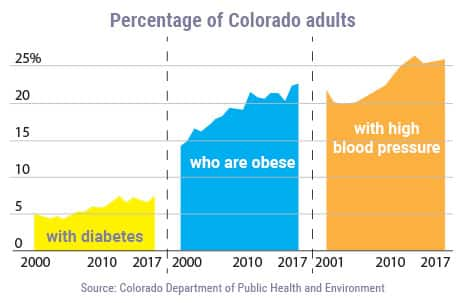
The box below reveals the surge in cardiovascular risk factors in Colorado, a state associated with healthier behavioral patterns than the southeast United States.
Heart Disease in Middle-Aged Men
A front-page article in the Wall Street Journal described surging numbers of heart attacks occurring in people living in Colorado, many of whom are physically active, but nonetheless have multiple cardiovascular risk factors.28
The article described many victims including a 55-year-old man who died of an acute heart attack. This prompted his group of friends to have checkups. Eleven of his friends had arterial issues and needed stents or other therapy.
Six of these 11 men with silent coronary artery disease played on an amateur hockey team. This was common amongst other Coloradoans who were physically active, but failed to control blood pressure, lipids/glucose, body weight and other heart-health practices.
A startling statistic discussed in the Wall Street Journal article portends a frightening future: More than 25% of elementary-school children screened in the 2018-2019 school year were overweight or obese. And 19.2% had borderline or high cholesterol.
High LDL cholesterol and its atherogenic subfractions, like apolipoprotein B, in early life predispose to vascular diseases in mid- to later life.29,30
A Colorado Springs cardiologist was quoted as regularly seeing men and women in their 30s and 40s with heart problems, such as high blood pressure, irregular heart rhythms, and heart attacks. This doctor noted how rare this was when he began his cardiology practice in the early 2000s.
Cardiovascular screening is now urged by public health officials, which is what most readers of Life Extension® magazine do each year with comprehensive blood tests.
When the researchers of this 2016 JAMA study controlled for:
- Diabetes,
- Hypertension,
- Cholesterol/triglycerides, and
- Kidney function...
…there was no longer a difference between obese and normal weight people for risk of coronary heart disease and stroke.
While this is encouraging, the researchers discovered that severely obese individuals had a nearly four-fold increase in heart failure, even when conventional risk factors (like blood pressure, glucose, and lipids) were considered.
The researchers pointed to evidence that excess body weight increases the heart’s workload. They also pointed to the role of fat cells in the belly (abdomen) releasing inflammatory factors that further damage the heart.
None of these studies measured critical additional blood factors that contribute to coronary artery disease, ischemic stroke, and heart failure.
If these added artery-clogging factors (like C-reactive protein and apolipoprotein B) were measured in type II diabetics and/or obese individuals, there would be an opportunity for more substantial reductions in cardiovascular diseases.
Too Many Needless Deaths
The studies reported in this editorial looked at conventional cardiovascular risk factors in overweight and diabetic individuals.
Up to 62% lower rates of cardiovascular events occurred in diabetics who achieved better control over their blood pressure, lipids, and blood sugar.
But what about the 38% risk for cardiovascular events that remained, even after controlling conventional risk factors?
As a reader of this magazine, you know there are about a dozenadditional cardiovascular factors such as homocysteine, apolipoprotein B, and hormone imbalances.
These blood markers should be measured, and efforts made to reduce them to safe ranges. This will likely yield greater reductions in cardiovascular events.
What Are Optimal Blood Levels of Apolipoprotein B?
Those with higher levels of a blood marker called apolipoprotein B are at greater risk for cardiovascular events.
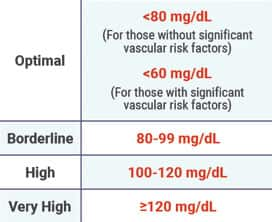
For people without preexisting vascular disease, diabetes or other risk factors, optimal apolipoprotein B is under 80 mg/dL.
Those at high arterial blockage risk should attempt to reduce apolipoprotein B to under 60 mg/dL. This will likely require dietary modifications and use of certain drug therapies.
When it comes to ideal apolipoprotein B levels, the lower the better. The following reference ranges reflect Life Extension’s general guidance for apolipoprotein B status when you get your blood test results back:
If your apolipoprotein B levels are not in optimal ranges, there are natural and pharmaceutical approaches to lowering them.
Now that cardiovascular disease is making a deadly comeback, it is imperative to have comprehensive blood tests, which is what most readers of this magazine do each year when they order the popular Male or Female Panels.
Annual Lab Test Sale
The high cost of blood tests prevents many people from testing for, and then optimizing, their cardiovascular risk factors.
We at Life Extension® recognized this problem 25 years ago.
Back in those days, many of our readers were challenged to persuade their doctors to order tests like homocysteine and hemoglobin A1c.
The price of blood tests in the 1990s was far higher than today.
This motivated us to develop a program that enables readers to order low-cost tests and then visit a blood draw station in their area at their convenience.
Blood test results come back in less than a week and are promptly emailed and mailed.
If there are any questions, our Wellness Specialists are available to assist, seven days a week, at no charge.
Once a year we discount prices of all lab tests. This serves as a convenient reminder to have one’s annual assessments performed at the lowest prices.
The extensive array of blood tests included in the Male and Female Panels can be viewed on the page to your right.
The discounted price for this year’s Male or Female Blood Panels (that includes apolipoprotein B and newly added ferritin) is $224. It’s a bit higher now than in years past, but it includes more important measures that cost over $2,000 at commercial labs.
To order the Male or Female Panel today, call 1-800-208-3444 or log on to: www.LifeExtension.com/blood
You can then visit a blood draw station we refer you to in your area at your convenience.
For longer life,
William Faloon
Blood Tests Identify Reversible Cancer Risks
Most people have annual blood tests to check for cardiovascular risk factors like total cholesterol, LDL and triglycerides.
What few realize is that other blood tests such asfasting insulin,31-34 glucose,35-39 and C-reactive protein40-45 are robustly associated with one’s future cancer risk.
Those who procrastinate about having comprehensive blood tests miss out on opportunities to correct risk factors before onset of cancer, dementia. kidney failure and cardiovascular diseases.
Blood Test Super Sale
Since our founding over 40 years ago, Life Extension® has urged its readers to have annual blood tests.
The number of lives saved by our recommendations is huge, including men diagnosed with early-stage prostate cancer who are readily cured. And many of today’s curative prostate treatments have far fewer side effects.
We have identified tens of thousands of people with elevated cardiovascular risk markers, allowing them to take corrective measures before an ischemic stroke or heart attack strikes.
The retail price throughout the year for these comprehensive Male or Female Panels is $299. These same tests at commercial labs cost over $2,000.
Just once a year, we discount the prices of all blood tests, enabling readers to obtain the Male or Female Blood Test Panels for only $224.
This represents almost a 90% savings compared to commercial lab prices.
To order a Male and/or Female Panel at the year’s lowest prices, call 1-800-208-3444 (24 hours) or log on to: www.LifeExtension.com/blood
References
- Carroll MD, Lacher DA, Sorlie PD, et al. Trends in serum lipids and lipoproteins of adults, 1960-2002. JAMA. 2005 Oct 12;294(14):1773-81.
- Collaboration NCDRF. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet. 2017 Jan 7;389(10064):37-55.
- Hopstock LA, Bonaa KH, Eggen AE, et al. Longitudinal and secular trends in total cholesterol levels and impact of lipid-lowering drug use among Norwegian women and men born in 1905-1977 in the population-based Tromso Study 1979-2016. BMJ Open. 2017 Aug 21;7(8):e015001.
- CDC. Centers for Disease Control and Prevention. Achievements in Public Health, 1900-1999: Tobacco Use — United States, 1900-1999. MMWR. 1999;48(43):986-93.
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019 Sep 10;140(11):e596-e646.
- Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005 Mar 31;352(13):1293-304.
- Mensah GA, Wei GS, Sorlie PD, et al. Decline in Cardiovascular Mortality: Possible Causes and Implications. Circ Res. 2017 Jan 20;120(2):366-80.
- Available at: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm4830a1.htm. Accessed March 2, 2021.
- Hartley A, Marshall DC, Salciccioli JD, et al. Trends in Mortality From Ischemic Heart Disease and Cerebrovascular Disease in Europe: 1980 to 2009. Circulation. 2016 May 17;133(20):1916-26.
- Moran AE, Forouzanfar MH, Roth GA, et al. Temporal trends in ischemic heart disease mortality in 21 world regions, 1980 to 2010: the Global Burden of Disease 2010 study. Circulation. 2014 Apr 8;129(14):1483-92.
- Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_05-508.pdf. Accessed March 2, 2021.
- Available at: https://www.cdc.gov/nchs/fastats/obesity-overweight.htm. Accessed February 28, 2021.
- Available at: https://www.cdc.gov/diabetes/data/statistics/statistics-report.html. Accessed March 2, 2021.
- Benjamin EJ, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019 Mar 5;139(10):e56-e528.
- Prevalence of Peripheral Neuropathy in Prediabetes. Diabetes. 2018;67(Supplement 1):552-P.
- Available at: https://www.hopkinsmedicine.org/news/media/releases/small_nerve_fibers_defy_neuropathy_conventions. Accessed March 2, 2021.
- Melsom T, Schei J, Stefansson VT, et al. Prediabetes and Risk of Glomerular Hyperfiltration and Albuminuria in the General Nondiabetic Population: A Prospective Cohort Study. Am J Kidney Dis. 2016 Jun;67(6):841-50.
- Tabak AG, Herder C, Rathmann W, et al. Prediabetes: a high-risk state for diabetes development. Lancet. 2012 Jun 16;379(9833):2279-90.
- Plantinga LC, Crews DC, Coresh J, et al. Prevalence of chronic kidney disease in US adults with undiagnosed diabetes or prediabetes. Clin J Am Soc Nephrol. 2010 Apr;5(4):673-82.
- Available at: https://www.medicalnewstoday.com/articles/304528.php. Accessed March 5, 2021.
- Sidney S, Go AS, Jaffe MG, et al. Association Between Aging of the US Population and Heart Disease Mortality From 2011 to 2017. JAMA Cardiology. 2019;4(12):1280-6.
- Curtin SC. Trends in Cancer and Heart Disease Death Rates Among Adults Aged 45-64: United States, 1999-2017. Natl Vital Stat Rep. 2019 May;68(5):1-9.
- Wong ND, Zhao Y, Patel R, et al. Cardiovascular Risk Factor Targets and Cardiovascular Disease Event Risk in Diabetes: A Pooling Project of the Atherosclerosis Risk in Communities Study, Multi-Ethnic Study of Atherosclerosis, and Jackson Heart Study. Diabetes Care. 2016 May;39(5):668-76.
- Gaede P, Lund-Andersen H, Parving HH, et al. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008 Feb 7;358(6):580-91.
- Vazquez-Benitez G, Desai JR, Xu S, et al. Preventable major cardiovascular events associated with uncontrolled glucose, blood pressure, and lipids and active smoking in adults with diabetes with and without cardiovascular disease: a contemporary analysis. Diabetes Care. 2015 May;38(5):905-12.
- Wong ND, Patao C, Malik S, et al. Preventable coronary heart disease events from control of cardiovascular risk factors in US adults with diabetes (projections from utilizing the UKPDS risk engine). Am J Cardiol. 2014 Apr 15;113(8):1356-61.
- Ndumele CE, Matsushita K, Lazo M, et al. Obesity and Subtypes of Incident Cardiovascular Disease. J Am Heart Assoc. 2016 Jul 28;5(8).
- Available at: https://www.wsj.com/articles/heart-disease-strikes-back-across-the-u-s-even-in-healthy-places-11579015880. Accessed March 2, 2021.
- Robinson JG, Williams KJ, Gidding S, et al. Eradicating the Burden of Atherosclerotic Cardiovascular Disease by Lowering Apolipoprotein B Lipoproteins Earlier in Life. Journal of the American Heart Association. 2018;7(20):e009778-e.
- Pletcher MJ, Bibbins-Domingo K, Liu K, et al. Nonoptimal lipids commonly present in young adults and coronary calcium later in life: the CARDIA (Coronary Artery Risk Development in Young Adults) study. Ann Intern Med. 2010 Aug 3;153(3):137-46.
- Stolzenberg-Solomon RZ, Graubard BI, Chari S, et al. Insulin, glucose, insulin resistance, and pancreatic cancer in male smokers. JAMA. 2005 Dec 14;294(22):2872-8.
- Shu X, Wu L, Khankari NK, et al. Associations of obesity and circulating insulin and glucose with breast cancer risk: a Mendelian randomization analysis. Int J Epidemiol. 2019 Jun 1;48(3):795-806.
- Ghanavati M, Rahmani J, Rinaldi G, et al. Fasting Insulin and Risk of Cancer Related Mortality in Non-diabetic Adults: A Dose-response Meta-analysis of Cohort Studies. Curr Diabetes Rev. 2020;16(4):357-63.
- Tsujimoto T, Kajio H, Sugiyama T. Association between hyperinsulinemia and increased risk of cancer death in nonobese and obese people: A population-based observational study. Int J Cancer. 2017 Jul 1;141(1):102-11.
- Stattin P, Bjor O, Ferrari P, et al. Prospective study of hyperglycemia and cancer risk. Diabetes Care. 2007 Mar;30(3):561-7.
- Michaud DS, Fuchs CS, Liu S, et al. Dietary glycemic load, carbohydrate, sugar, and colorectal cancer risk in men and women. Cancer Epidemiol Biomarkers Prev. 2005 Jan;14(1):138-47.
- Gapstur SM, Gann PH, Lowe W, et al. Abnormal glucose metabolism and pancreatic cancer mortality. Jama. 2000 May 17;283(19):2552-8.
- Jee SH, Ohrr H, Sull JW, et al. Fasting serum glucose level and cancer risk in Korean men and women. Jama. 2005 Jan 12;293(2):194-202.
- Lajous M, Willett W, Lazcano-Ponce E, et al. Glycemic load, glycemic index, and the risk of breast cancer among Mexican women. Cancer Causes Control. 2005 Dec;16(10):1165-9.
- Li Y, Zhong X, Cheng G, et al. Hs-CRP and all-cause, cardiovascular, and cancer mortality risk: A meta-analysis. Atherosclerosis. 2017 Apr;259:75-82.
- Han Y, Mao F, Wu Y, et al. Prognostic role of C-reactive protein in breast cancer: a systematic review and meta-analysis. Int J Biol Markers. 2011 Oct-Dec;26(4):209-15.
- Wang G, Li N, Cao L, et al. Association between the level of high sensitivity C-reactive protein and risk of breast cancer among non-diabetic females: a prospective study in Kailuan group. Zhonghua Zhong Liu Za Zhi. 2014 Dec;36(12):944-8.
- Peres LC, Mallen AR, Townsend MK, et al. High Levels of C-Reactive Protein Are Associated with an Increased Risk of Ovarian Cancer: Results from the Ovarian Cancer Cohort Consortium. Cancer Res. 2019 Oct 15;79(20):5442-51.
- Pastorino U, Morelli D, Leuzzi G, et al. Baseline and postoperative C-reactive protein levels predict mortality in operable lung cancer. Eur J Cancer. 2017 Jul;79:90-7.
- Shrotriya S, Walsh D, Nowacki AS, et al. Serum C-reactive protein is an important and powerful prognostic biomarker in most adult solid tumors. PLoS One. 2018;13(8):e0202555.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun